Minimally invasive aortic valve replacement (MIAVR)
Share This Post Minimally invasive aortic valve replacement (MIAVR) is a surgical procedure used to replace a diseased or damaged aortic valve with an artificial
Minimally invasive aortic valve replacement (MIAVR) is a surgical procedure used to replace a diseased or damaged aortic valve with an artificial valve. It is called “minimally invasive” because it involves smaller incisions and less trauma to the patient compared to traditional open-heart surgery.
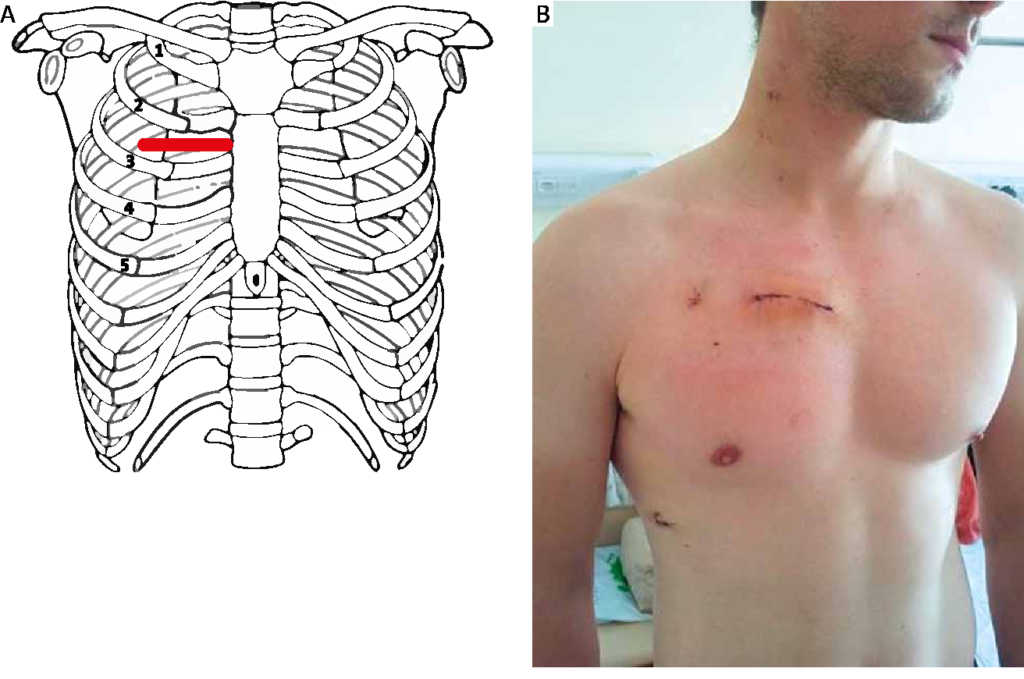
During MIAVR, the surgeon accesses the heart through small incisions in the chest, typically between the ribs, instead of making a large incision in the sternum (breastbone) as in traditional open-heart surgery. This approach allows for a more cosmetic result, reduced pain, shorter hospital stays, and faster recovery times.
The surgical techniques used in MIAVR can vary depending on the surgeon’s expertise and the specific case. One common approach is called a mini-sternotomy, in which a small incision is made in the upper part of the sternum. Another approach is a right anterior thoracotomy, where an incision is made on the right side of the chest between the ribs.
Once the incisions are made, the surgeon uses specialized instruments and a video-assisted system to access and replace the aortic valve. The damaged valve is removed, and an artificial valve, either mechanical or bioprosthetic, is inserted and secured in place. The surgeon then closes the incisions, and the patient is taken to the recovery area.
Minimally invasive aortic valve replacement offers several advantages over traditional open-heart surgery, including:
Indications
Minimally invasive aortic valve replacement (MIAVR) may be considered as a treatment option for patients with certain indications. The specific indications can vary depending on the surgeon’s expertise and the patient’s individual case, but here are some common indications for MIAVR:
Contraindications
While minimally invasive aortic valve replacement (MIAVR) offers several advantages, there are also certain contraindications that may make a patient unsuitable for this procedure. Some common contraindications for MIAVR include:
Share This Post Minimally invasive aortic valve replacement (MIAVR) is a surgical procedure used to replace a diseased or damaged aortic valve with an artificial
Share This Post Minimally invasive Surgery involve accessing the heart through small incisions, typically between the ribs or through the sternum (breastbone). This approach offers